
Structure of Heart – Final Year MBBS Notes
Structure of Heart – Final Year MBBS Advanced Notes
📑 Table of Contents
- 1. Overview
- 2. External Features
- 3. Chambers of Heart
- 4. Valves
- 5. Conducting System
- 6. Coronary Circulation
- 7. Nerve Supply
- 8. Histology
- 9. Embryology Basics
- 10. Relations of Heart
- 11. Cardiac Cycle (Mechanism)
- 12. Clinical Correlations
- 13. High‑Yield Exam Points
- 14. Mnemonics
- 15. FAQs
- 16. Quick Revision Summary
- 17. Conclusion
- 18. Recommended Resources
🔬 Overview
The heart is a muscular pump that maintains unidirectional blood flow through the circulatory system. In final year, a deep understanding of its structure – gross, microscopic, and developmental – is essential for correlating with clinical syndromes. The heart lies in the middle mediastinum, oriented obliquely with apex directed leftward and downward.
🔍 External Features
- Base (posterior): formed mainly by left atrium, receives pulmonary veins.
- Apex: formed by left ventricle, lies at left 5th intercostal space midclavicular line.
- Surfaces: sternocostal (anterior – right ventricle), diaphragmatic (inferior – left ventricle), pulmonary (left – left ventricle).
- Borders: right border (right atrium), inferior border (right ventricle), left border (left ventricle), superior border (atria and great vessels).
- Sulci: coronary (atrioventricular) sulcus, anterior and posterior interventricular sulci – contain coronary arteries and veins.
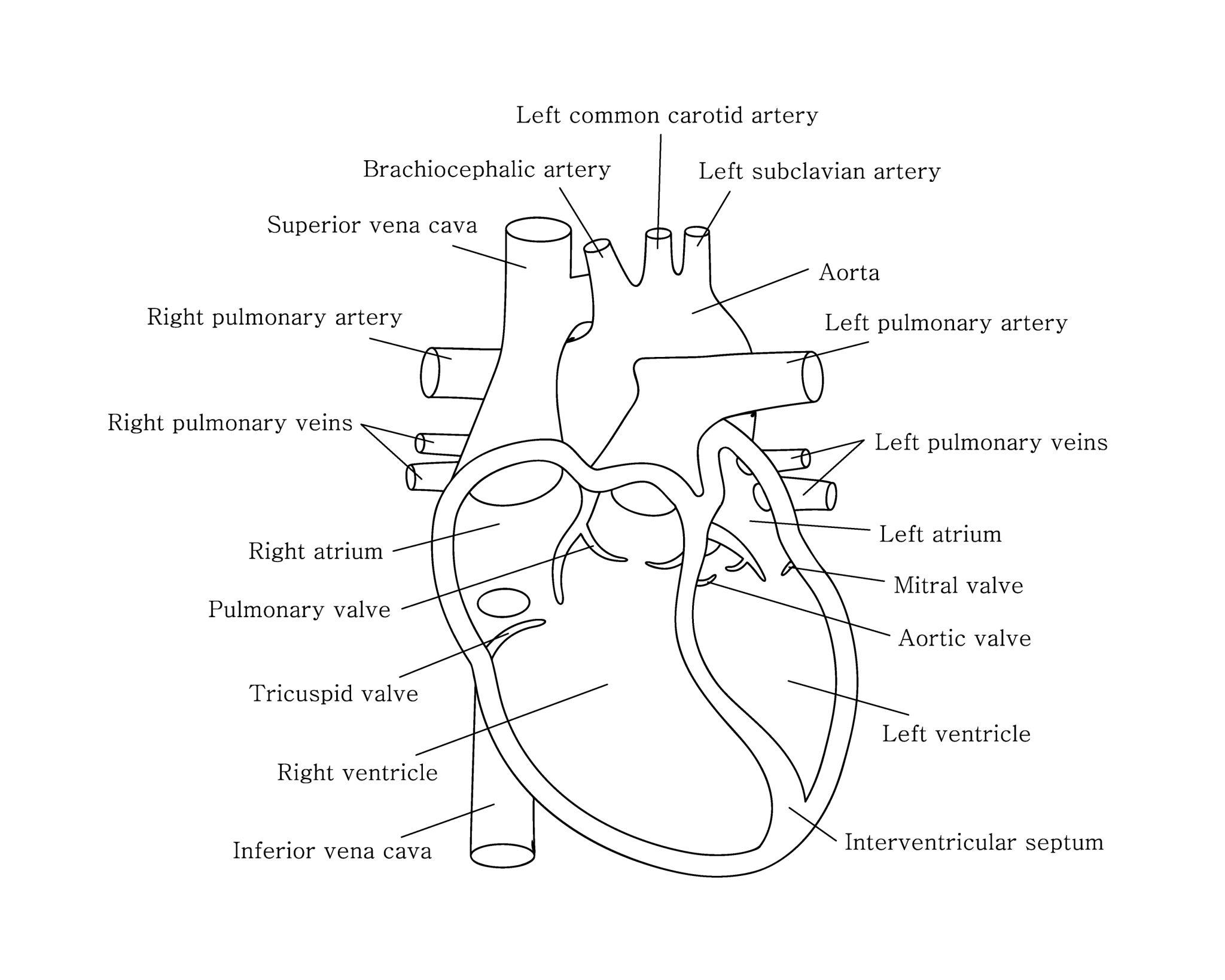
🏠 Chambers of Heart
Right Atrium
Parts: sinus venarum (smooth posterior) and pectinate muscles (rough anterior). Crista terminalis separates them. Openings: SVC, IVC, coronary sinus, and right atrioventricular orifice. Fossa ovalis (remnant of foramen ovale).
Right Ventricle
Inflow tract with trabeculae carneae, papillary muscles (anterior, posterior, septal), and chordae tendineae attached to tricuspid valve. Outflow tract (infundibulum) leads to pulmonary valve. Septomarginal trabecula (moderator band) carries part of the right bundle branch.
Left Atrium
Smooth walled except for pectinate muscles in the auricle. Receives four pulmonary veins. Interatrial septum has fossa ovalis on right side.
Left Ventricle
Thickest chamber (systemic pump). Two large papillary muscles (anterior, posterior) attached to mitral valve via chordae. Walls are trabeculated but finer than right ventricle. Aortic vestibule leads to aortic valve.
🚪 Valves of the Heart
- Tricuspid valve: three cusps (anterior, posterior, septal), right AV orifice.
- Mitral valve (bicuspid): two cusps (anterior, posterior), left AV orifice.
- Aortic valve: three semilunar cusps (right, left, posterior/non‑coronary).
- Pulmonary valve: three semilunar cusps (anterior, right, left).
Chordae tendineae and papillary muscles prevent valve prolapse during systole.
⚡ Conducting System
- Sinoatrial (SA) node: located in right atrium near SVC opening – primary pacemaker.
- Internodal tracts: anterior, middle, posterior – conduct impulse to AV node.
- Atrioventricular (AV) node: in interatrial septum near coronary sinus.
- Bundle of His: penetrates fibrous skeleton, divides into right and left bundle branches.
- Purkinje fibers: subendocardial network in ventricles.
🩸 Coronary Circulation
Arteries: Right coronary artery (RCA) – supplies right atrium, right ventricle, SA node (60%), AV node (80%), posterior descending artery (in right dominant heart). Left main coronary artery divides into left anterior descending (LAD) and left circumflex (LCx). LAD supplies anterior wall and septum; LCx supplies lateral wall.
Venous drainage: Coronary sinus (great, middle, small cardiac veins) → right atrium. Anterior cardiac veins drain directly.
Dominance: defined by artery giving posterior descending artery (RCA dominant ~70%, left dominant ~10%, codominant ~20%).
🔌 Nerve Supply
Sympathetic: from cervical and upper thoracic ganglia – increases heart rate and contractility. Parasympathetic: via vagus nerve – decreases heart rate (SA/AV nodes). Visceral afferent fibres (pain) travel with sympathetic to spinal cord levels T1‑T4.
🔬 Histology of Heart
- Endocardium: endothelial lining + subendothelial connective tissue.
- Myocardium: cardiac muscle fibers (striated, branched, one central nucleus, intercalated discs).
- Epicardium (visceral pericardium): mesothelium + fibroelastic tissue.
- Fibrous skeleton: dense connective tissue around valves and orifices, electrically insulates atria from ventricles.
🧬 Embryology Basics
Heart develops from mesoderm (cardiogenic region). Paired endocardial tubes fuse to form primitive heart tube. Cardiac looping (day 23‑28) creates the basic shape. Septation of atria, ventricles, and outflow tract occurs by growth of membranous and muscular ridges. Common congenital defects (VSD, ASD, tetralogy of Fallot) relate to errors in septation.
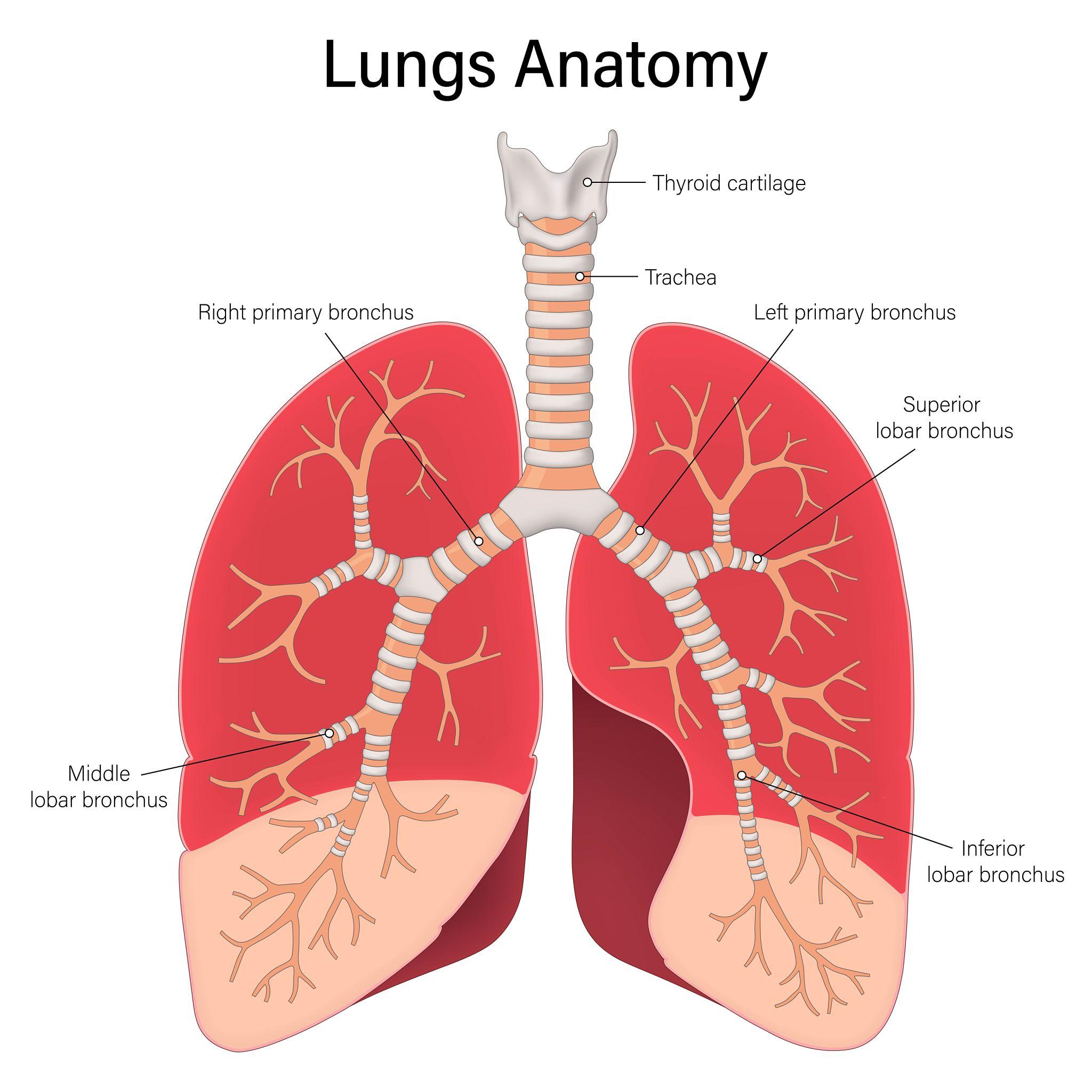
🌬️ Relations of Heart
The heart is surrounded by the pericardium and sits in the middle mediastinum. Anterior: sternum, ribs, and lungs (covered by pleura). Posterior: esophagus, descending aorta, vertebral column. Lateral: lungs (right and left) with phrenic nerves passing anterior to hilum.
The phrenic nerves run anterior to the lung roots and innervate the diaphragm; they are closely related to the pericardium.
🔄 Mechanism – Cardiac Cycle
The cardiac cycle consists of systole (contraction) and diastole (relaxation).
- Atrial systole: completes ventricular filling.
- Isovolumetric contraction: all valves closed, pressure rises.
- Rapid ejection: semilunar valves open, blood ejected.
- Reduced ejection: ventricular pressure falls.
- Isovolumetric relaxation: all valves closed, pressure drops.
- Rapid filling: AV valves open, ventricles fill.
- Diastasis: slow filling.
Pressure and volume changes correlate with heart sounds (S1, S2) and ECG.
🏥 Clinical Correlations
- Coronary artery territories: LAD occlusion → anterior MI; RCA → inferior MI; LCx → lateral MI.
- Valvular lesions: aortic stenosis (systolic murmur), mitral regurgitation (pansystolic), mitral stenosis (diastolic).
- Heart blocks: first‑degree (PR >200ms), second‑degree (Mobitz I/II), third‑degree (complete dissociation).
- Congenital defects: VSD (left‑to‑right shunt), tetralogy of Fallot (VSD, overriding aorta, RVH, pulmonary stenosis).
- Cardiac tamponade: fluid in pericardium → muffled sounds, hypotension, distended neck veins (Beck’s triad).
📌 High‑Yield Exam Points
- Coronary dominance: RCA gives PDA in 70%.
- SA node blood supply: RCA (60%) or LCx (40%).
- Moderator band (septomarginal trabecula) – contains right bundle branch.
- Aortic valve cusps: right, left, non‑coronary.
- Layers: endocardium, myocardium, epicardium; fibrous skeleton insulates.
- Fossa ovalis – remnant of foramen ovale.
- Papillary muscles prevent valve prolapse.
🧩 Mnemonics
Coronary arteries: “LAD supplies the anterior wall, RCA supplies the inferior (right) wall.”
Heart valves order (from right to left): “Try Pulling My Aorta” – Tricuspid, Pulmonary, Mitral, Aortic.
Branches of left main: “LAD and LCx” (LAD = Left Anterior Descending, LCx = Left Circumflex).
Layers of heart: “Endo, Myo, Epi” (inside to outside).
AV node location: “Koch’s triangle” – bordered by tendon of Todaro, coronary sinus orifice, septal leaflet of tricuspid.
❓ Frequently Asked Questions
📝 Quick Revision Summary
- Chambers: RA (sinus venarum, pectinate), RV (trabeculae, moderator band), LA (smooth), LV (thick wall).
- Valves: tricuspid, mitral, aortic, pulmonary – supported by chordae/papillary muscles.
- Conducting system: SA node → AV node → His → Purkinje.
- Coronaries: RCA (right, inferior), LAD (anterior, septum), LCx (lateral).
- Nerve supply: sympathetic (increase HR), parasympathetic (decrease HR).
- Histology: three layers, fibrous skeleton.
- Relations: anterior to sternum, posterior to esophagus, lateral to lungs.
🎯 Conclusion
A thorough grasp of cardiac structure is indispensable for clinical practice, especially in cardiology, critical care, and surgery. This guide consolidates the essential details needed for final year exams and beyond. Regular review with atlases and clinical cases will cement this knowledge.
📚 Recommended Resources
| Resource Name | Topic | Link |
|---|---|---|
| Gray's Anatomy for Students | Comprehensive cardiac anatomy | # |
| Netter's Atlas of Human Anatomy | Heart illustrations | # |
| Clinical Anatomy by Snell | Applied anatomy of heart | # |
| Harrison's Principles of Internal Medicine | Cardiovascular disorders | # |
| Robbins & Cotran Pathologic Basis of Disease | Heart pathology | # |
| Embryology by Langman | Heart development | # |
| Echo in Clinical Practice (online) | Echocardiography correlation | # |
🔎 Secondary Keywords: cardiac anatomy coronary circulation heart chambers conducting system heart valves clinical cardiology
📌 Long‑tail Keywords: final year MBBS heart anatomy notes high yield cardiac structure heart relations and mediastinum embryology of heart for medical students